

Small clinics face a specific problem that enterprise healthcare IT guides do not address. The numbers published for large hospital EHR implementations — $500,000 to several million dollars — do not reflect the reality of a 3-physician family practice or a single-specialty urgent care center. The cost structure is different. The compliance requirements are the same. And the vendor options are often mismatched to the actual need.
This guide gives small clinic owners and practice managers a grounded cost breakdown for 2026: what custom EHR development actually costs at your scale, what drives prices up, where savings are real, and what questions to ask before signing a contract.
What is custom EHR software?
Custom EHR (Electronic Health Record) software is a patient data management system built specifically for a clinic’s workflows, specialty, and compliance requirements. Unlike off-the-shelf platforms, it integrates only the modules a practice needs and connects directly to existing billing, lab, and scheduling tools without forcing workflow changes.
What drives EHR development cost for small clinics
Six factors account for most of the cost variance between a $40,000 build and a $90,000+ build. Understanding them lets you scope your project accurately before getting vendor quotes.
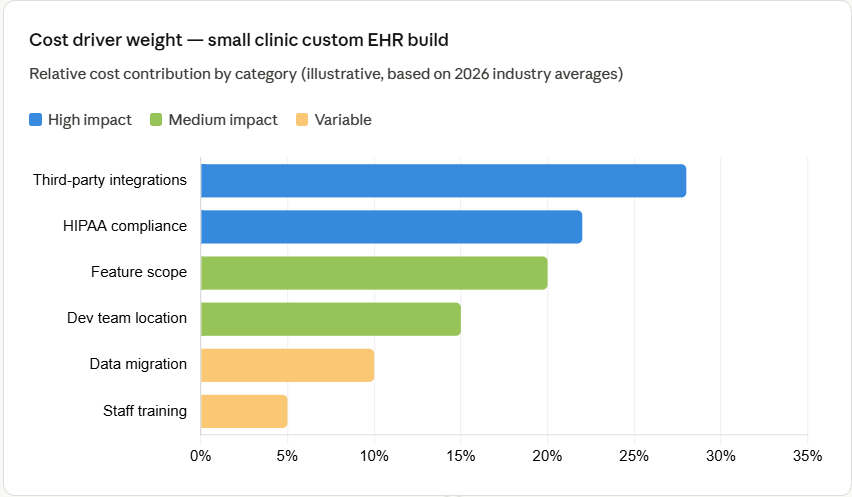
Third-party integrations — lab systems, billing software, e-prescribing platforms, and imaging tools — account for the largest single cost variable. Each connected system requires custom API work. At $10,000 to $30,000 per integration (Arkenea, 2026), a clinic connecting four external systems adds $40,000 to $120,000 to its base build cost alone.
HIPAA compliance is not optional. Every custom EHR requires role-based access controls, audit logging, encryption at rest and in transit, and a signed Business Associate Agreement with every vendor touching patient data. Clinics that underestimate compliance infrastructure consistently face cost overruns of 25% or more post-launch.
Cost breakdown by development tier
Custom EHR projects for small clinics fall into three tiers based on feature scope and deployment complexity. The table below maps each tier to its typical cost range, timeline, and best-fit clinic type.
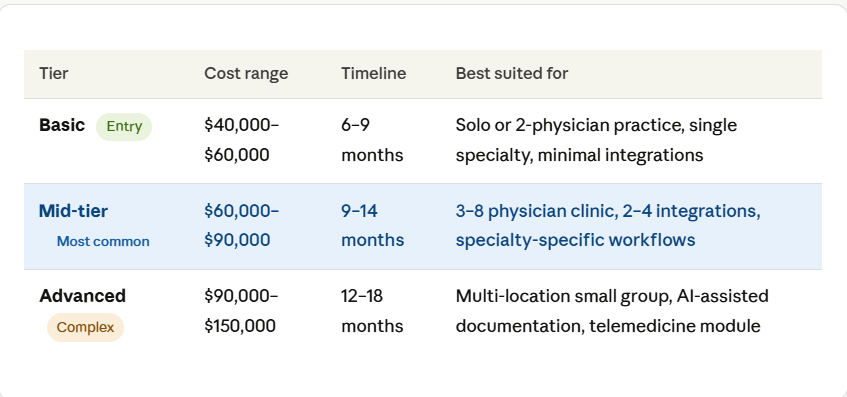
The mid-tier range covers most independent specialty clinics in 2026. A 5-physician orthopedic practice connecting to a lab system, a billing platform, and an e-prescribing tool will typically land between $65,000 and $85,000 for a custom build, based on current development rates for US-experienced offshore teams (Galaxy Weblinks, 2026).
HIPAA compliance in EHR development means building a system that meets the US Health Insurance Portability and Accountability Act’s Privacy and Security Rules. This includes encrypting patient health information, enforcing access controls, maintaining audit logs, and ensuring every vendor with data access has a signed Business Associate Agreement. Non-compliance carries tiered fines starting at $100 per violation under the HITECH Act enforcement framework.
Component-level cost breakdown
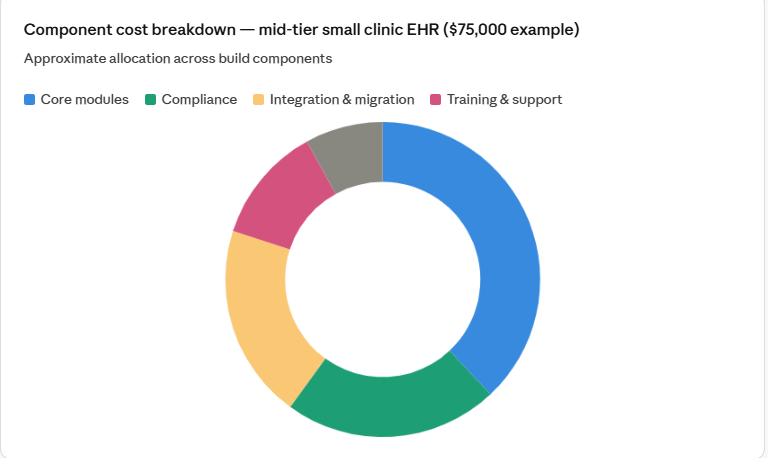
A custom EHR is not a single product. It is a collection of modules, each with its own development, testing, and compliance cost. Below is a component-level breakdown for a mid-tier small clinic build in 2026.
| Component | Cost range | Notes |
|---|---|---|
| Patient records module | $8,000–$15,000 | Demographics, medical history, allergy tracking |
| Appointment scheduling | $5,000–$10,000 | Multi-provider calendar, reminders, waitlist |
| Clinical documentation | $8,000–$18,000 | SOAP notes, templates, e-signature |
| E-prescribing (EPCS) | $6,000–$12,000 | DEA-compliant, formulary checks |
| Billing integration | $8,000–$20,000 | ICD-10, CPT coding, clearinghouse API |
| HIPAA compliance layer | $10,000–$20,000 | RBAC, audit logs, encryption, BAA setup |
| Lab/imaging integration | $8,000–$25,000 | Per connected system, HL7/FHIR API work |
| Data migration | $5,000–$15,000 | From paper or legacy EHR to new system |
| Staff training | $2,000–$8,000 | Per-user cost scales with clinic size |
| Annual maintenance | $7,500–$18,000/yr | 15–20% of build cost; ongoing after launch |
Custom build vs off-the-shelf: where the cost math changes
Off-the-shelf EHR platforms like eClinicalWorks (starting at $449/month per provider) or DrChrono ($249/month) appear cheaper at the start. Over a five-year window, the total cost of ownership often reverses for clinics with specialty-specific workflows or complex integration needs.
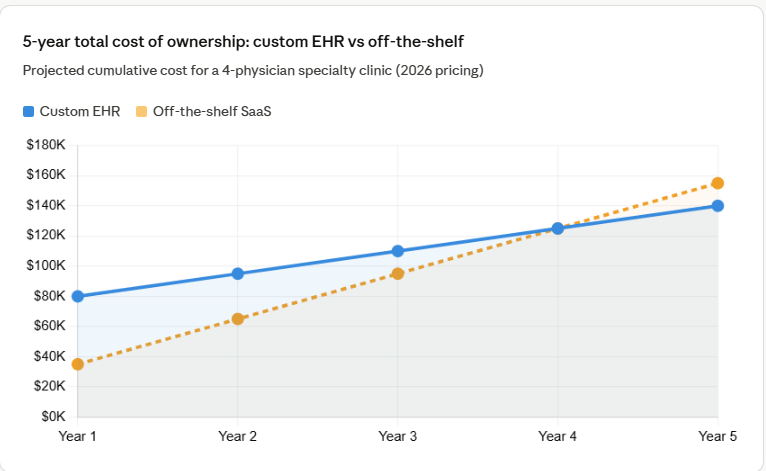
Off-the-shelf costs compound through subscription escalation, per-provider add-on fees, customization surcharges, and integration middleware costs. A 4-physician clinic paying $599/month per provider for a combined EHR and practice management subscription spends $28,752 per year before any customization. Add mandatory support tiers, data storage overages, and third-party integration connectors, and the annual cost reaches $35,000 to $50,000 per year at scale.
Annual EHR maintenance typically consumes 15–20% of the original build cost (Stats Market Research, 2026). A $75,000 custom build carries an ongoing maintenance obligation of $11,250–$15,000 per year. This must be included in any five-year budget comparison against subscription platforms.
What changed in 2026: three cost factors that did not exist in 2023
Three developments since 2023 have materially changed the cost structure of custom EHR builds for small clinics.
1. FHIR R4 interoperability is now mandatory
CMS Interoperability Rules effective since 2021 require certified EHR systems to support HL7 FHIR R4 APIs for patient data access. In 2026, building FHIR-compliant APIs into a custom EHR from scratch adds $8,000–$15,000 to development cost. Skipping FHIR compliance disqualifies a system from Medicare and Medicaid program participation.
2. AI-assisted documentation is now a buyer expectation
Ambient AI scribes that generate clinical notes from voice have shifted from enterprise feature to small clinic expectation in 2026. Adding an AI documentation module to a custom EHR build adds $12,000–$25,000 depending on the vendor API chosen (Amazon HealthScribe, Nuance DAX, or custom LLM integration).
3. Cloud-first deployment is the default
Cloud-based EHR systems now hold an 86.49% share of the global EHR market (Fortune Business Insights, 2026). For small clinics, this means lower upfront hardware costs but higher recurring cloud infrastructure costs. A clinic that previously spent $30,000–$60,000 on on-premise server infrastructure now pays $800–$2,400 per month for equivalent cloud hosting, a trade that benefits most small practices on a 3-year horizon.
Using pre-built, ONC-certified HIPAA-compliant components instead of fully custom modules for standard features (patient registration, scheduling, basic documentation) saves $50,000–$150,000 compared to building from scratch, according to implementation data from Taction Software (2026). Custom development then focuses only on specialty-specific workflows where differentiation actually matters.
Geography impact on development cost
Where your development team is located is the single largest lever on build cost after feature scope. The rate difference between a US-based team and an India-based healthcare-specialized team can reduce total project cost by 40–60% without reducing output quality, provided the offshore team has documented healthcare software experience.
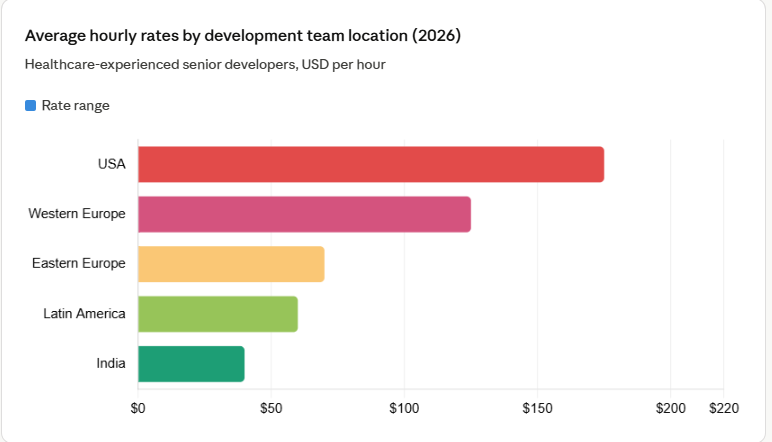
For a mid-tier EHR build requiring 1,200 development hours, the cost difference between a US team at $175/hour ($210,000) and an India-based healthcare team at $40/hour ($48,000) is $162,000. That gap closes when accounting for project management overhead, timezone communication costs, and revision cycles, but healthcare-experienced offshore teams consistently deliver 50–60% savings for small clinic projects in 2026.
Five questions to ask any EHR development vendor before signing
| Question | What a strong answer looks like |
|---|---|
| Do you have prior HIPAA-certified EHR builds in production? | Named client references, not just general healthcare experience |
| How do you handle FHIR R4 API compliance? | Pre-built certified components, not built from scratch each time |
| What does the maintenance contract cover after launch? | Specific SLA response times, security patch schedule, scope definition |
| Who owns the source code after delivery? | Full code ownership transferred to the clinic at final payment |
| How is data migration handled from our current system? | Defined migration protocol, test environment, rollback plan |
Realistic budget planning for small clinic EHR in 2026
A small clinic building a custom EHR in 2026 should budget for three phases: build, launch, and the first two years of operation. The build cost is a one-time investment. Maintenance, cloud hosting, and training updates are ongoing obligations that most first-time buyers underestimate by 30–40%.
The most defensible budget approach for independent clinics is a phased build: start with core patient records, scheduling, and documentation modules, then add integrations and specialty features in year two. This approach reduces upfront capital requirement while allowing the team to validate workflows before committing full development spend.
For clinics weighing custom development against off-the-shelf platforms, the decision turns on one variable: workflow specificity. If a practice’s clinical workflows match what a major EHR vendor offers out of the box, off-the-shelf platforms are the cost-effective choice for the first three years. If specialty workflows require significant modification or the practice has integration requirements that standard platforms handle poorly, custom development pays back within three to four years for most small clinic operations.