


A founder-level cost guide covering MVPs, full platforms, compliance overhead, and the build-vs-white-label decision that determines your year-one budget.
Most telemedicine cost guides quote a $30,000 to $300,000 range and leave founders to figure out the rest. That range is technically accurate and practically useless. A mental health startup validating a direct-to-consumer therapy model has nothing in common with a multi-specialty urgent care group building a provider dashboard with EHR integration.
This guide segments the real cost of telemedicine app development by startup type, build path, and feature set. Every figure is sourced from 2026 industry data. The goal is a budget you can defend to your investors and a scope you can hand to a development partner.
What is telemedicine app development?
Telemedicine app development is the process of building a digital platform that connects patients with healthcare providers through video, voice, or asynchronous messaging. It includes patient-facing and provider-facing interfaces, HIPAA-compliant video infrastructure, appointment scheduling, and integrations with billing, pharmacy, and EHR systems. Cost and complexity vary sharply based on feature scope and compliance requirements.
| Basic MVP range
$40K–$70K Single platform, core features
|
Mid-tier platform
$80K–$150K EHR + e-Rx + cross-platform
|
Enterprise build
$200K–$500K+ AI, RPM, full integration
|
Market CAGR (2025–30)
17.55% Grand View Research, 2025
|
The three build paths health startups actually use
Before breaking down feature costs, the most important decision is which build path your startup will take. This single choice determines your year-one budget range more than any individual feature.
| White-label platform
$5K–$50K upfront + monthly fees Pre-built, rebranded fast. Vendors like Doxy.me, SimplePractice, or VSee. Launch in weeks. Limited differentiation, vendor lock-in risk.
|
Most common for seed/Series A
Custom MVP first $40K–$100K, 3–6 months Core consultation workflow built custom. Validates demand before full platform spend. Scales into full build with proven traction.
|
Full custom platform
$150K–$500K+, 9–18 months Full architecture ownership. Needed for multi-specialty, AI-assisted, or enterprise-grade deployments. Justified post-Series A with defined product roadmap.
|
White-label solutions cut launch timelines by roughly 50% compared to custom builds. For most health startups at seed stage, the right move is white-label to validate, then custom to scale. Attempting a full custom platform before proving demand is the most common budget mistake in the telehealth startup category.
What is an MVP in telemedicine app development?
A telemedicine MVP (Minimum Viable Product) is a stripped-down version of a telehealth platform that covers only the core consultation workflow: patient registration, appointment booking, HIPAA-compliant video call, and basic post-visit documentation. It excludes EHR integration, e-prescribing, and advanced analytics. An MVP lets founders validate patient demand before committing to full platform spend.
Cost by startup type: what founders in each vertical actually pay
Telemedicine cost varies more by startup type than by any other variable. A mental health platform and a dermatology asynchronous diagnosis tool share almost no infrastructure. Below are realistic cost profiles by vertical, based on 2026 build data.
| Startup type | Typical build cost | Timeline | Key cost driver |
|---|---|---|---|
| Mental health / therapy platform DTC | $40K–$80K | 3–5 months | HIPAA video + async messaging + provider matching |
| Urgent care telehealth MVP B2C | $55K–$90K | 4–6 months | E-prescribing (EPCS), pharmacy routing, fast patient intake |
| Multi-specialty group platform B2B2C | $100K–$180K | 6–10 months | Multi-provider routing, EHR integration, insurance billing |
| Pediatric / chronic care RPM IoT | $120K–$250K | 8–14 months | IoT device integration, real-time vitals, care team dashboards |
| AI-first diagnostics platform AI | $200K–$400K+ | 12–18 months | ML model training, clinical decision support, FDA pre-submission |
A real-world example: a three-physician urgent care group in Texas built a telemedicine MVP covering patient intake, video consultation, and post-visit prescription routing, with no EHR integration, for a total of $58,000 in 11 weeks. This is the realistic floor for a functional, HIPAA-compliant product in 2026.
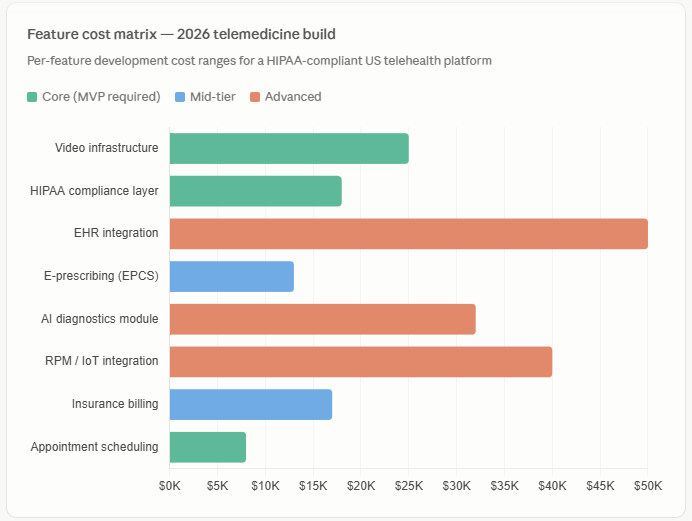
Feature-level cost breakdown
Every feature in a telemedicine app carries a development cost, a compliance cost, and a maintenance cost. Health startup founders who budget only for development discover the other two categories after launch. Below is a feature-level breakdown for 2026.
Custom bidirectional integrations with legacy EHR systems requiring proprietary connectors can reach $80,000 or more, and the EHR vendor’s integration approval and credentialing process can add 8 to 20 weeks on top of development time. Founders who plan EHR integration should budget 6 to 12 months total for a live connection with a major system like Epic or Cerner.
HIPAA compliance is non-negotiable in the US, and failing an audit can cost six figures in fines. Legal counsel, compliance consulting, and regular audits should be factored in from day one. Most early-stage telehealth startups spend $5,000 to $25,000 on their first compliance review, with annual re-certification adding $5,000 to $10,000 per year on top of that (TelehealthTech, 2026).
The real costs founders discover after launch
Development cost is the visible line item. The table below shows the ongoing cost structure that shapes whether a telehealth startup reaches profitability in year two or runs out of runway.
| Cost category | Monthly range | Notes |
|---|---|---|
| HIPAA-compliant cloud hosting (AWS / GCP / Azure healthcare tier) | $2,000–$10,000+ | Scales with traffic and data volume |
| Video API (Twilio Video / Daily.co with BAA) | $500–$4,000 | Per-minute billing at scale; budget separately from infrastructure |
| E-prescribing network fees (Surescripts) | $300–$1,500 | Per-transaction model at high volume |
| Platform maintenance and bug fixes | $3,000–$8,000 | 15–20% of build cost annually; monthly estimate |
| State telehealth licensing (per provider, per state) | $500–$3,000 | Multi-state platforms face compounding licensing costs |
| Total post-launch operating cost (mid-tier platform) | $8,000–$25,000/mo | Before staffing; must be modeled in Series A runway |
A $2 per-visit video API fee seems minor until a platform scales to 5,000 visits a month. That becomes $10,000 monthly or $120,000 per year. Founders who model only development cost and ignore usage-based infrastructure pricing consistently underestimate year-two operating expenses by 40 to 60 percent.
5-year cost trajectory: custom build vs white-label
The white-label vs custom build decision is primarily a timing question. White-label platforms lower upfront cost and risk at seed stage. Custom builds deliver better unit economics at scale. The crossover point for most telehealth startups is between months 18 and 30.

A study from Health Recovery Solutions found that telehealth visits cost $40 to $50 compared to $136 to $176 for in-person visits, a saving of up to $126 per visit. For a practice averaging 200 virtual visits per month, that operating efficiency covers a meaningful portion of annual platform costs and makes the unit economics of a custom build compelling at scale.
The telemedicine software market has converged around a few dominant revenue models: per-consultation fee for DTC and marketplace models, monthly subscription per provider for B2B clinic tools, enterprise licensing for annual contracts, and freemium for base-tier access. For most modern platforms, subscription wins because it creates predictable recurring revenue and aligns incentives with customer success. Model your revenue path before finalizing build scope.
What a well-scoped telemedicine budget actually looks like
Health startups that control telemedicine development cost do three things differently from those that run over budget.
First, they fix scope before fixing price. A vendor quote on an undefined scope is a number with no meaning. Every feature decision, platform choice, and integration dependency must be confirmed in writing before a line of code is written.
Second, they phase the build. An MVP covering the consultation workflow launches in 3 to 5 months and costs $40,000 to $70,000. EHR integration, multi-provider routing, and AI features follow in phase two, funded by traction data from phase one. This approach reduces total year-one capital required by 40 to 60 percent compared to building everything upfront.
Third, they budget for compliance independently. HIPAA infrastructure, legal review, state licensing, and annual audits are not development costs. They are operating costs that begin on the first day patient data touches the platform. A telehealth startup that treats compliance as a one-time checkbox discovers the real bill when the first audit arrives.
More than 76% of patients now prefer telehealth visits over non-emergency in-person care. The demand is established. The cost of building a product to serve it is finite and calculable. The variable is not whether to build, but what to build, in which order, with which partner, and at which stage of your company.